








Mapping Malaria in Italy
Text by Andrea Bagnato
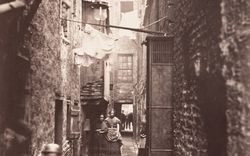
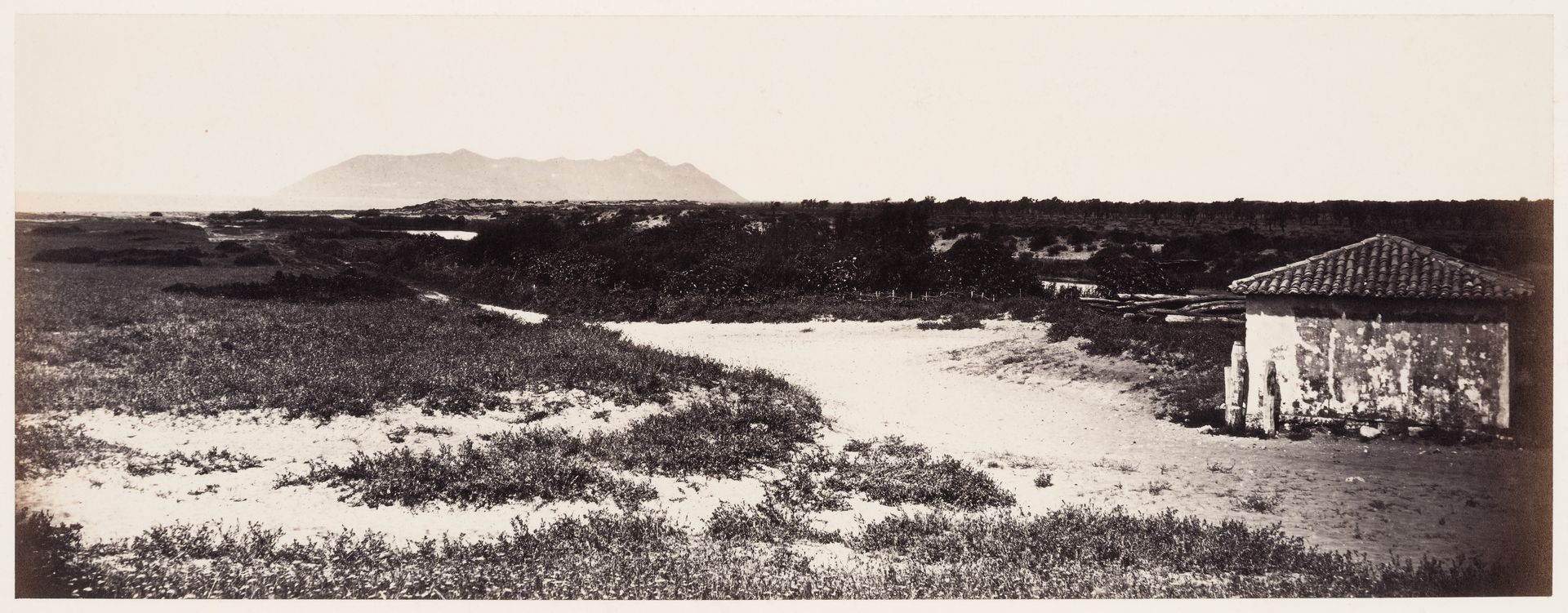
One of my persistent memories from the summers I spent in Sardinia as a boy is the rows upon rows of tall, pale eucalyptus trees and how oddly out of place they seemed amid the Mediterranean shrubs. Even more odd were the pools of putrid, stagnant water that still lie behind many of the island’s splendid beaches. Only much later did I learn to see this landscape as the product of centuries of human (and microbial) action. While I had previously thought of malaria as a disease of the “tropics,” I discovered that Sardinia suffered the highest malaria mortality rates in Western Europe well into the twentieth century. The “oddities” I observed in the landscape were the result of a long-term project to eliminate the disease.
Robert Macpherson, photographer. Pontine marshes at Badino, Monte Cercio in distance, Pontinia, Italy, ca. 1860s. CCA. PH1984:0520

Robert Macpherson, photographer. View of a lake and tower in Ninfa, Pontine Marshes, near Sermoneta, Italy, between 1858 and 1871. CCA. PH1982:0425:028

Robert Macpherson, photographer. View of a road with a town in the distance, Campagna di Roma, Italy, between 1851 and 1871. CCA. PH1987:0898
Since at least the Roman era and until the mid-twentieth century, malaria was endemic across Europe, and particularly deadly along the Mediterranean coast. Malaria parasites do not require a dense host population to survive because they are transmitted by Anopheles mosquitoes, which have a flight range of several kilometres. And because Anopheles mosquitoes breed in stagnant water, they are present mostly in fertile plains, along coasts, and around river basins. Consequently, malaria is a non-urban disease, uniquely interconnected with the conditions of the landscape and the patterns of its inhabitation. In contrast to more short-lived urban epidemics, malaria is a stable presence in space. It is no coincidence that Fernand Braudel considered it a key actor of the longue durée in Mediterranean history.1
Read more
Architecture and urban planning in the nineteenth century were greatly influenced by the principle of fluid circulation and the development of sanitation standards. Among others, Leonardo Benevolo has described the rise, from the 1840s, of hygienist movements within European urban planning in response to frequent epidemics of cholera and tuberculosis. Ildefons Cerdà’s plan for Barcelona is probably the best known materialization of such concerns.2 From a medical point of view, the notion of circulation emerged from the miasmatic theory, according to which the environment itself—noxious gases, putrid water, or air currents—was the cause of most infections.
-
Braudel introduced the concept of longue durée to look at history through the lens of long-term factors such as topography and climate. See Fernand Braudel, The Mediterranean and the Mediterranean World in the Age of Philip II, vol. I (London: Collins, 1972), 23-167. ↩
-
Leonardo Benevolo, The History of the City (London: Scolar, 1980), 755–770. ↩

Robert Macpherson, photographer. View of the Campagna di Roma, near the Frascati Railway, Italy, between 1851 and 1858. CCA. PH1987:0847
Michel Foucault aligned the modern management of epidemics, including that framed by miasmatic theory, with what he defined as the “apparatus of security.” Foucault argued that as of the late seventeenth century, European urban epidemics like smallpox and cholera were no longer dealt with through a binary division between healthy and sick—as had previously been the case with plague outbreaks—but rather through the quantification and management of risk across the entire population. Circulation, one such tool of management, is, according to Foucault, not restricted to urban space, but rather pertains to the milieu, a term that describes both the natural and urban realms. Modern biopolitics, in other words, is concerned with creating new landscapes that control the risk of infection.1
By expanding the focus to the non-urban, it becomes clear that architecture was only one of many technologies used to manage disease. The discovery and control of malaria in Italy proves, I think, one of Foucault’s central intuitions: that modernity reshaped not only the body, but also its entire environment. The concurrence of its establishment as a nation state with the emergence of its public health strategy makes Italy a unique case to understand how infectious disease control was central to the modern project.
-
Michel Foucault, Security, Territory, Population: Lectures at the Collège de France, 1977–1978 (New York: Picador, 2007), 4–23. ↩
Air
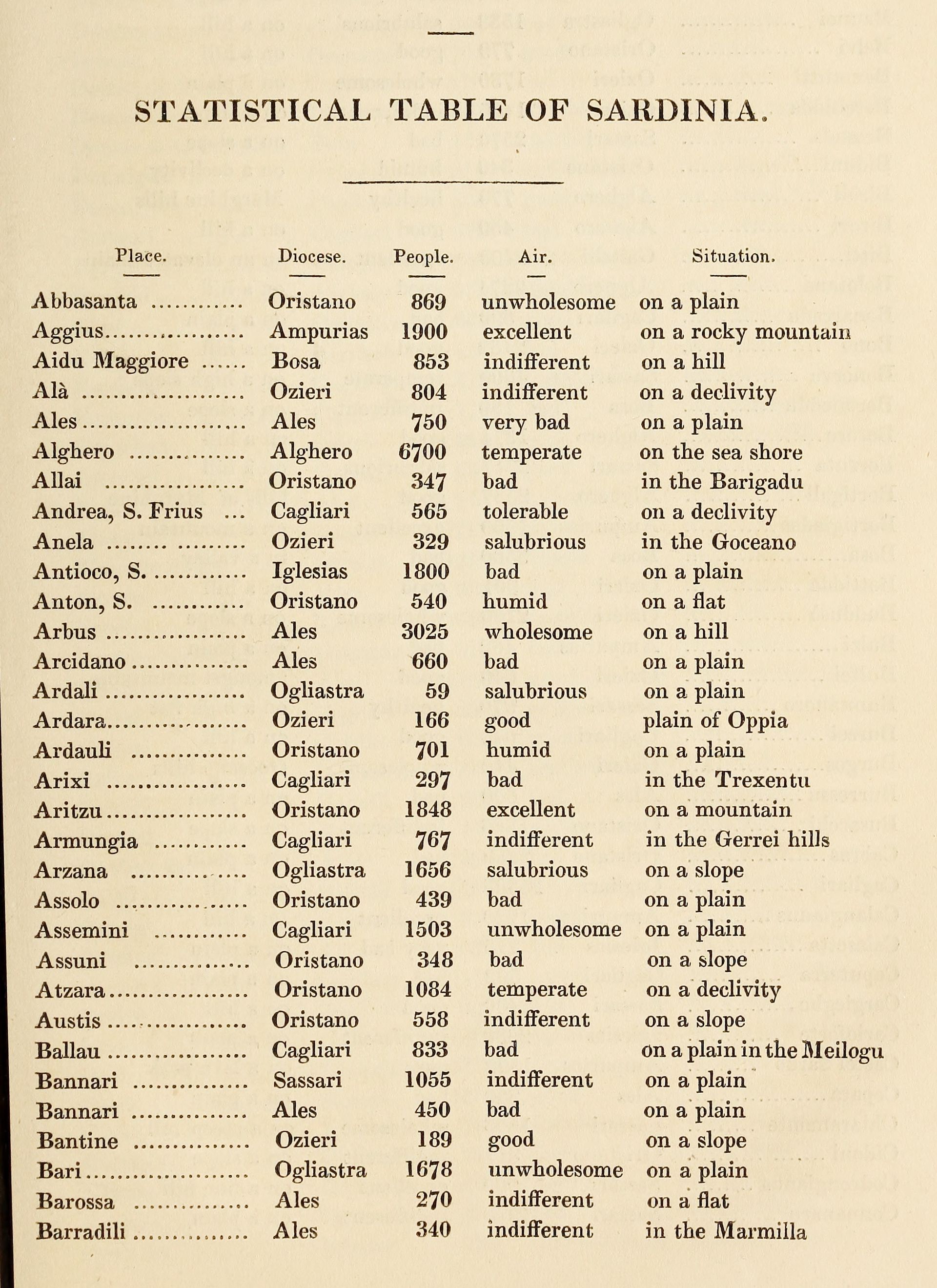
William H. Smyth, atlas of Sardinian air, in Sketch of the Present State of the Island of Sardinia (London: 1828)
Because of its distinctive symptoms, malaria has been documented empirically in Italy for centuries and mentioned in many travelogues. Until the 1880s, microorganisms were unknown and the prevalence of a given infection was considered a matter of geography. As with many epidemic diseases, malaria was most virulent in areas of widespread ecological disruption and exploitation, in this case due to coal mines, railways, and large agricultural estates (called latifundia). As a result, peasants, shepherds, and miners were disproportionately affected.
The first known quantification of malaria in an Italian region is presented in an 1828 book, Sketch of the Present State of the Island of Sardinia, written by English admiral William H. Smyth. After explaining the history and geography of the island, Smyth appends a “statistical table” of Sardinian towns in which he lists not only the population count of each, but also their topography and air quality, rated from “very bad” to “unwholesome” to “pure.” This was, of course, a proxy for the endemicity of malaria, viewed through the lens of miasmatic theory.1
Yet, when the Kingdom of Italy was proclaimed in 1861, the new Italian state was not aware of the national scale of the disease. Malaria was discovered, unexpectedly, through the establishment of Italy’s railways. The central purpose of the unification of Italy was to create a single economic area by abolishing the complex system of trade fees that existed among pre-unitary states. After unification, agriculture was reorganized: wheat cultivation was expanded in northern regions, while in the south it was replaced with olive and citrus trees. By allowing the circulation of produce and commodities throughout Italy, the railways allowed agriculture, which until then was mainly local, to enter the liberal capitalist system. The railways also connected Italy to continental European markets.2
Cover page of the report on malaria presented to the Italian Parliament by the prefecture of Trapani, Sicily, 14 February 1882. Archivio Storico del Senato, Rome
But railway construction was so slow that in 1878 the Italian Parliament commissioned an inquiry, directed by Senator Luigi Torelli. Torelli travelled across the peninsula to assess the state of the works and the causes of delay. He realized that railway workers were falling ill and dying at alarming rates, and that the cause was malaria. Torelli started to track worker mortality rates and found that malaria appeared to have become worse since unification. The raised embankments for the rail tracks prevented the drainage of rainwaters, creating new marshes along the Italian coasts. The demand for timber also accelerated the deforestation of the Apennine Mountains, further impairing the soil’s capacity to absorb water. Through his infrastructural survey, Torelli realized before others that malaria, infecting entire regions, was the single biggest impediment to the development of Italy.
In 1880, Torelli reported to Parliament that 45 percent of the nation’s railway lines lay in malarial areas and pressured lawmakers to gather accurate regional data. Under his direction, the Senate office distributed a questionnaire to all 259 provincial health councils, asking them to report on the situation of malaria in their territory and to represent malarial zones on a map through a standardized graphic system. The councils dutifully completed the questionnaires, but many pointed out that they did not possess a map of their own territory—a fact that Torelli had not considered. And the few maps that did exist were at wildly different scales and levels of detail, often hand drawn by local officials.1 To achieve a unified cartographic representation, Torelli enlisted the help of the newly created Military Geographic Institute (IGM), which provided a complete map of Italy, albeit at scales varying from 1:50,000 to 1:250,000. The 590 sheets supplied by IGM were again distributed to the health councils, each of which marked the extent of malaria before returning them.
-
The health council reports are held in the Senate’s archives in Rome; collectively, they make for a unique document of the premodern State. ↩
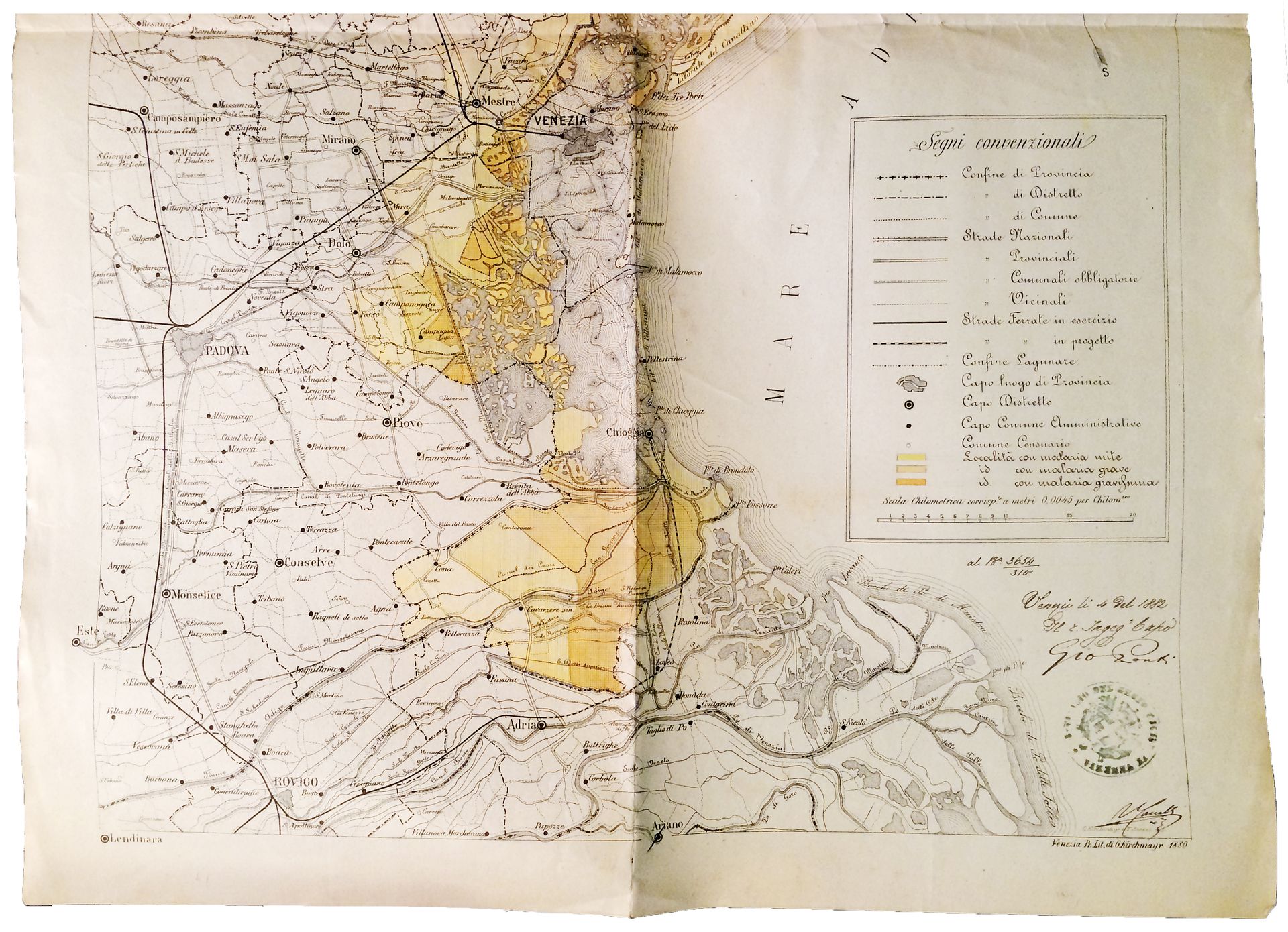
Map of malarial areas around Venice, 4 September 1882. Archivio Storico del Senato, Rome
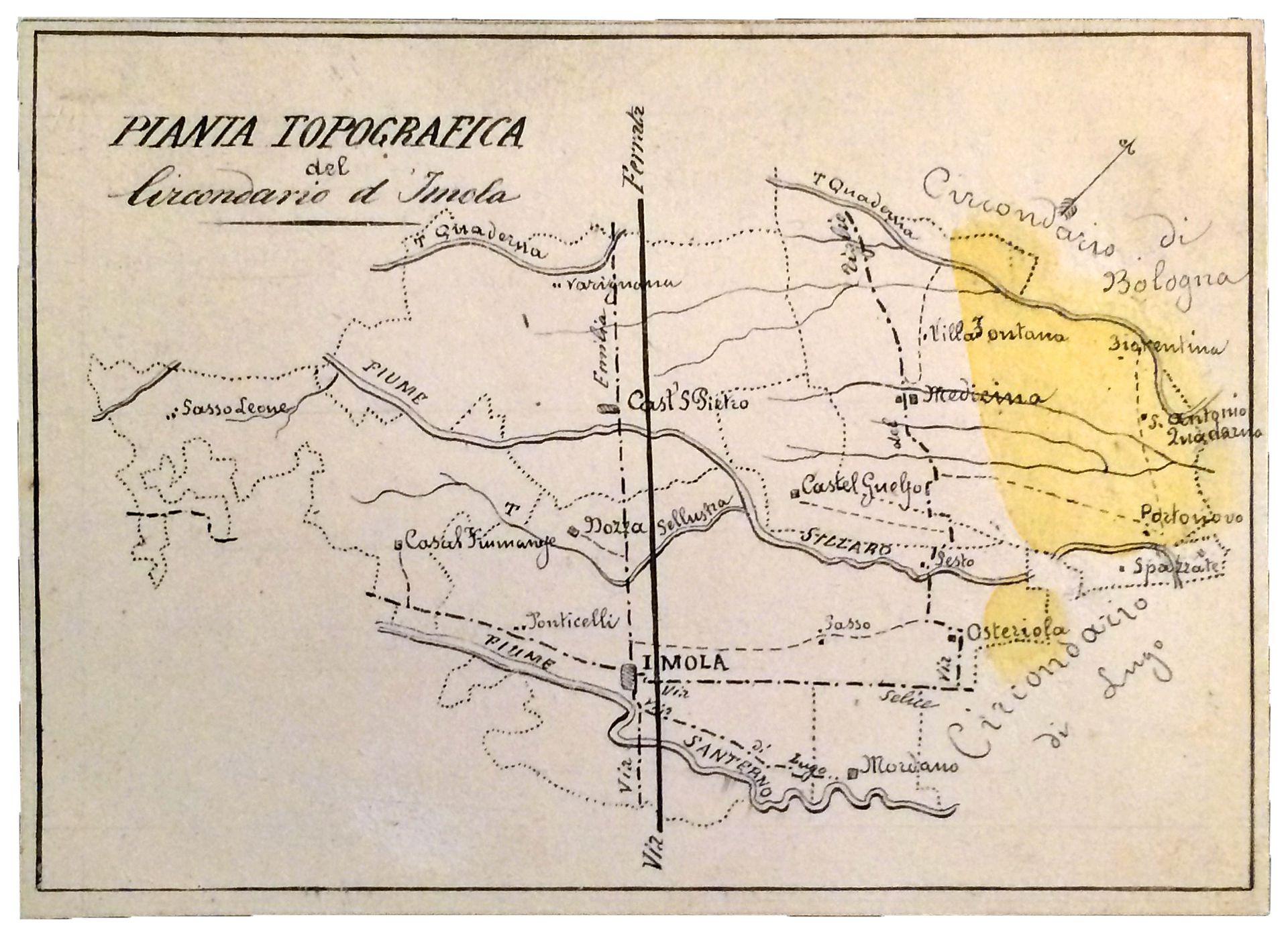
Map of malarial areas around Imola, 1881–82. Archivio Storico del Senato, Rome
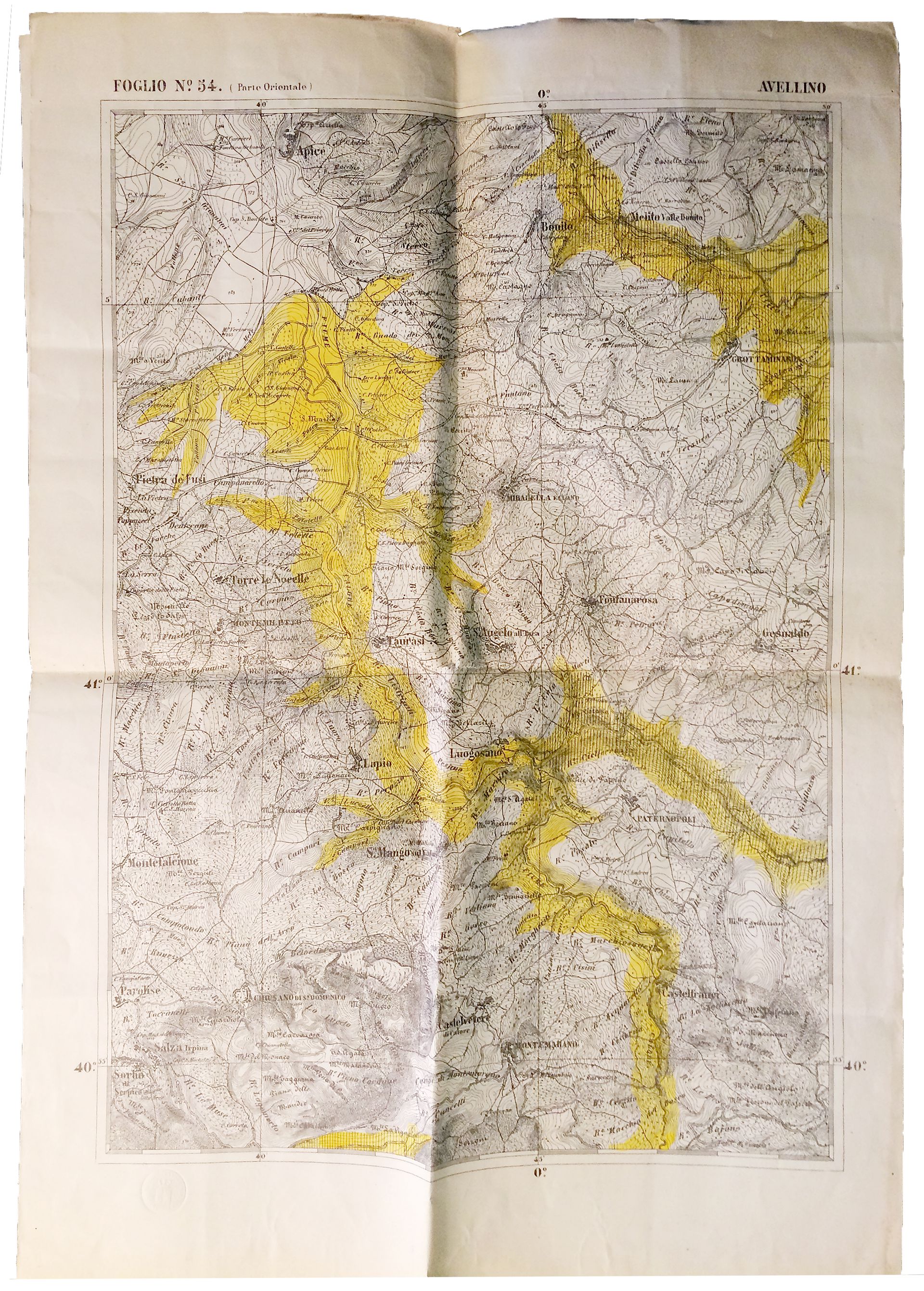
Map of malarial areas around Avellino, 27 February 1883. Archivio Storico del Senato, Rome
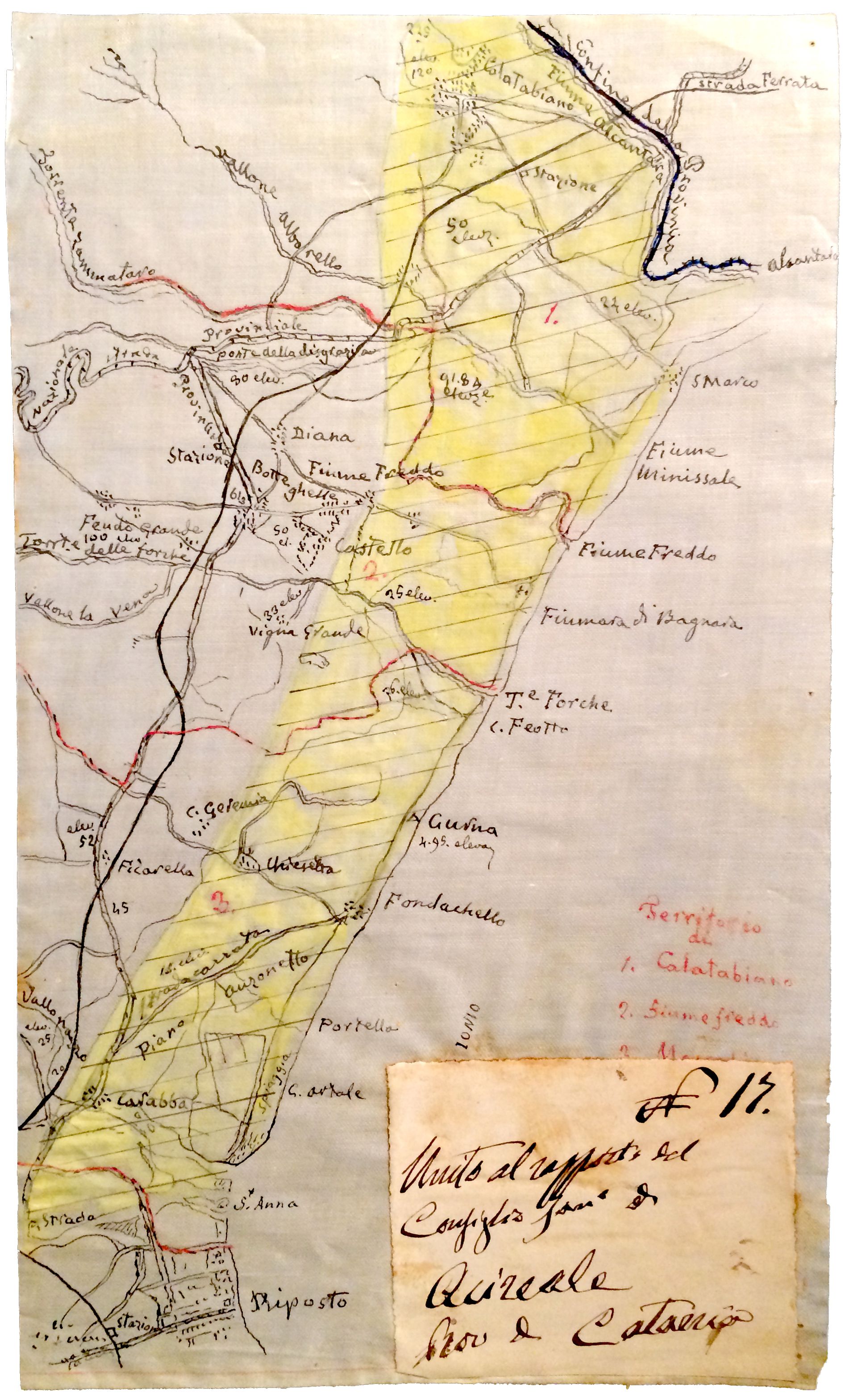
Map of malarial areas on the Sicilian coast around Acireale, 21 April 1881. Archivio Storico del Senato, Rome
Over the following two years, the Senate office painstakingly compiled the sheets into a single 1:1,000,000 scale chart—the first visual representation of malaria’s extent in Italy. Torelli presented the map to Parliament on 30 June 1882, defining it as “the basis of the operations to be undertaken against the great scourge” and using it to convince lawmakers that malaria could no longer be ignored.1 He went as far as to write an educational book, published as a paperback to maximize its distribution. The national map of malaria transformed a series of isolated reports into one event. What had been regarded as a private condition of peasant life suddenly became a public concern.2
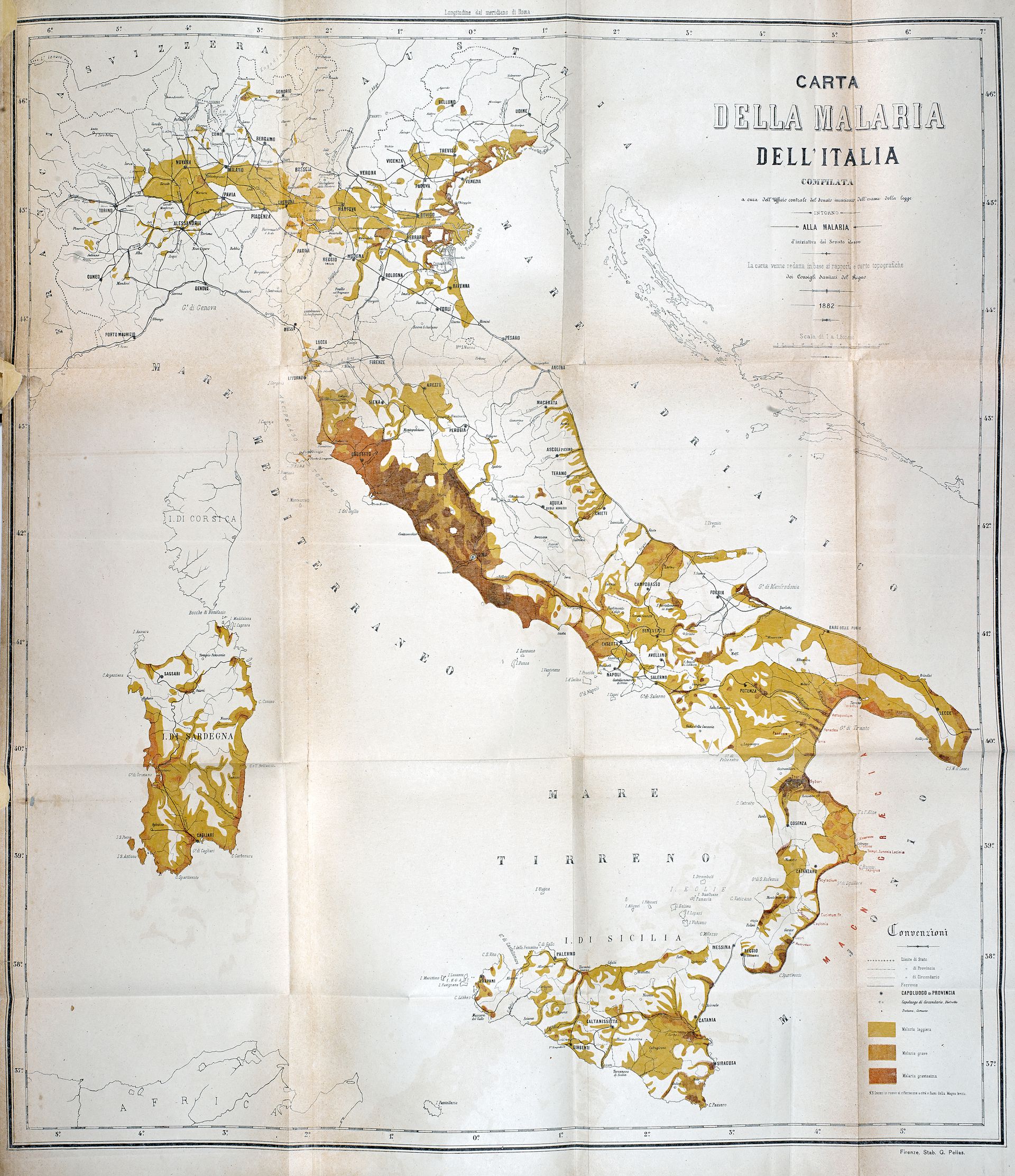
Luigi Torelli, map of malaria in Italy at the scale 1:1,500,000, reproduced in Carta della malaria dell’Italia (Florence: 1882)
In adopting semi-quantitative methods, Torelli was very likely influenced, on the one hand, by the emergence of medical geography as a discipline—August Hirsch’s landmark text, Handbook of Geographical and Historical Pathology, was published in 1881—and on the other, by the increased systematization of statistics. His work, in particular, encouraged the collection of health statistics in Italy, which began officially in 1887.1
Torelli’s malaria map represents the confluence of a series of nation-building processes: cartographic surveys, the gathering of population data, and the construction of a railway network. James Scott has famously described the advance of the modern state as a process of making its territories and peoples legible.2 In the case of Italy this was also true for pathogens. The very figure of Luigi Torelli—not a physician, but a statesman and public servant who had also worked with Ferdinand de Lesseps to promote the Suez Canal—reveals that malaria was not (yet) a problem of public health but, rather, one of infrastructure.
Land

New farmhouses built on reclaimed swamplands, north of Venice, c. 1920-1935
Torelli’s work succeeded in mobilizing the Italian Parliament. The political and medical elite agreed that the reclamation of swamplands was the only way to reduce the spread of malaria—since, in their opinion, the infective agent was the water itself, drainage would put an end to miasmatic exhalations. As early as 1882, the Parliament passed the Legge Baccarini, the first law authorizing large-scale land reclamation (called bonifica), as a matter of national interest. It is during this period that thousands of eucalyptus trees, erroneously thought capable of absorbing excess water from the soil, were imported from Australia and planted along roads and railways as a form of localized hygienic protection.
At the same time, the map of malaria was a dramatic representation of Italy’s internal differences. Undoubtedly, it contributed to the idea that Italy was divided into an advanced North and a backwards South—itself a modern construct. This view was compounded by the many parliamentary reports on what came to be called the questione meridionale, or the Southern Question. In order to maintain its position of economic advantage in what was a semi-colonial relationship, the North medicalized the landscape of the South (and its inhabitants) and fashioned it as the “Other.”
The reclamation of coastal plains in central and southern Italy had the explicit goal of converting infected land to productive cultivation. Environmental historian Marco Armiero has pointed out that the use of bonifica should be framed within a broader strategy of the liberal state to assert itself in untamed portions of its territory and bring the natural resources of those regions (soil and water) under capitalist control. In Armiero’s words, “The South became the open laboratory for the new technocratic approach to the economic and ecological problems of the country.”1
-
Marco Armiero, A Rugged Nation: Mountains and the Making of Modern Italy (Cambridge: White Horse, 2011), 36. ↩
Parasites
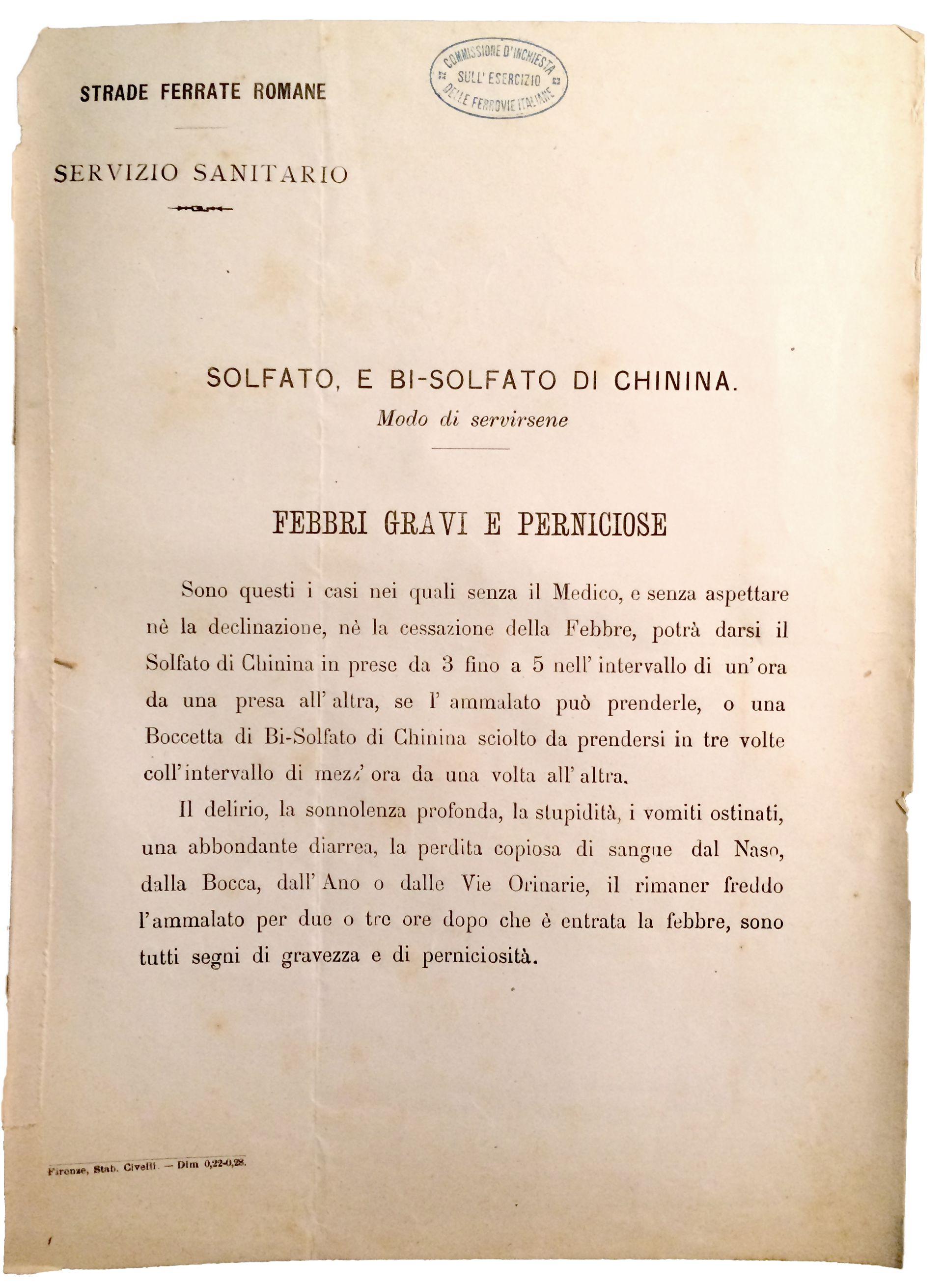
Instructions for the treatment of acute malaria using quinine by the Roman Railways Health Services. Quinine was distributed to all their employees in 1879, a measure which was later implemented across Italy. Archivio Storico del Senato, Rome
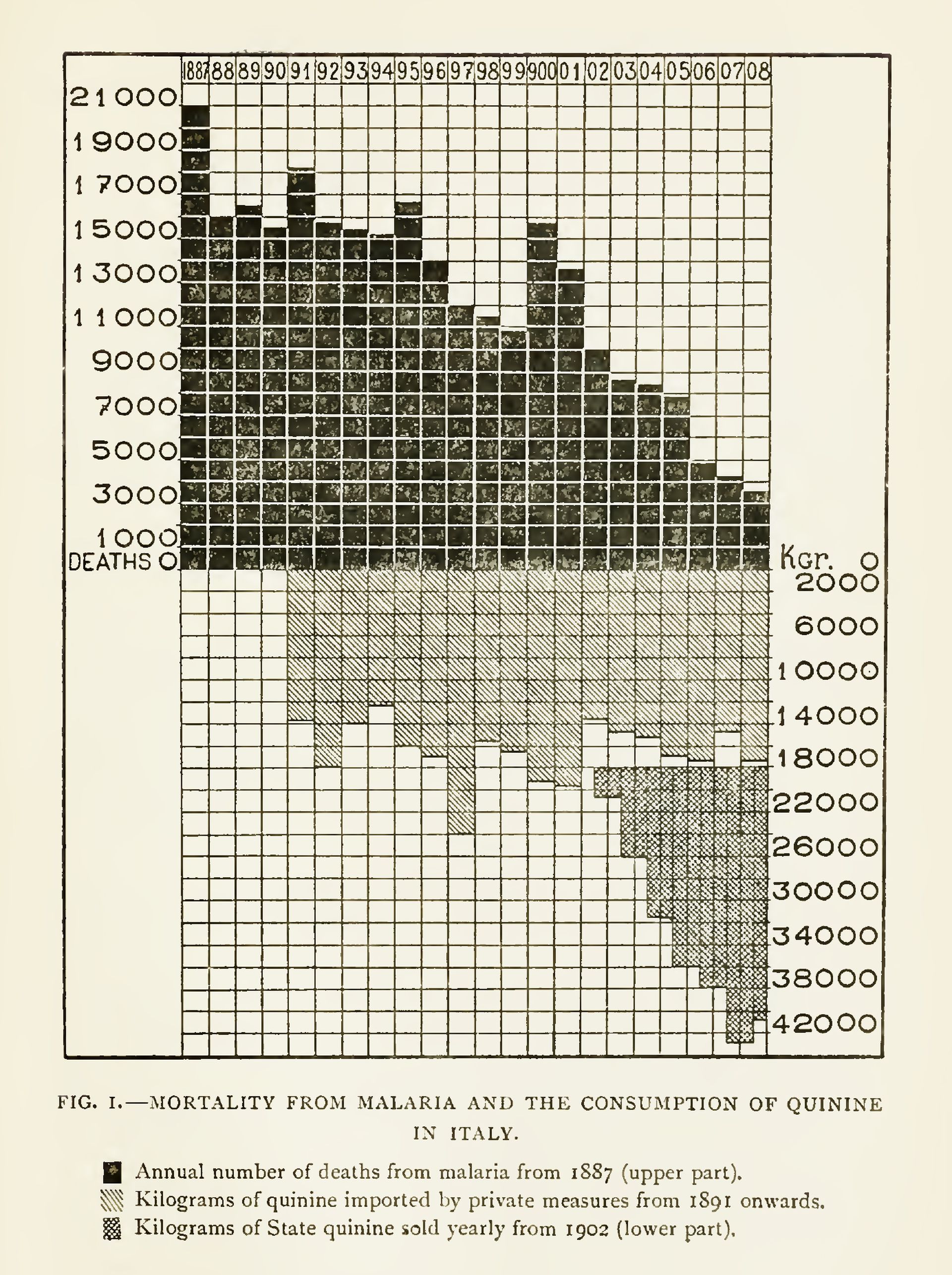
Angelo Celli, malariologist. A graph showing the decline of malaria deaths in Italy in relation to the growing use of quinine, in Ronald Ross, The Prevention of Malaria (New York: 1910), 451
Meanwhile, in 1884, a staggering discovery by Alphonse Laveran, a French military doctor, revealed that malaria was caused by microscopic blood parasites. And fifteen years later, Ronald Ross and Giovanni Battista Grassi found that it was mosquitoes, not miasmas, that transmitted the parasite, finally explaining the nexus between swamps and malaria. With malaria redefined as a vector-borne disease, malariology became an institutionalized discipline, and one in which Italian scientists maintained global authority until the late 1930s. The Society for the Study of Malaria was founded in Rome in 1898, funded not only by the state, but also by railway and agrarian companies.
From this point on, malaria control measures progressively reduced in scale, evolving into a set of standards and prescriptions. The Italian Parliament took the radical step of nationalizing the supply of quinine and distributing it at no cost to everyone living or working in malarial zones. The state also undertook massive information campaigns to educate Italians on the protocols of quinine use, and on the measures to make homes mosquito-proof. A pamphlet published in 1905 instructs, among other things: to screen every door and window; to sleep under a bed net; not to sit outside chatting in the evenings; and, if the latter was unavoidable, to cover one’s head and face in full.1 As can be imagined, the population did not accept these measures unanimously (it was reported that the state-distributed bed nets were reused to make tomato sauce) and took many years to assimilate them.2 Slowly but steadily, malaria mortality rates started to decrease. As Bruno Latour pointed out, since malaria could not be tackled by means of a simple vaccination, it was “to be destroyed . . . by ordering the colonists and natives to build their houses differently, to dry up stagnant ponds, to build walls of different materials, or to alter their daily habits.”3
-
Società per gli Studi della Malaria, Istruzioni popolari per difendersi dalla malaria (Rome: 1905). ↩
-
Frank M. Snowden, The Conquest of Malaria: Italy, 1900–1962 (New Haven and London: Yale University Press, 2006), 73–75. ↩
-
Bruno Latour, The Pasteurization of France (Cambridge, MA: Harvard University Press, 1988), 144. ↩
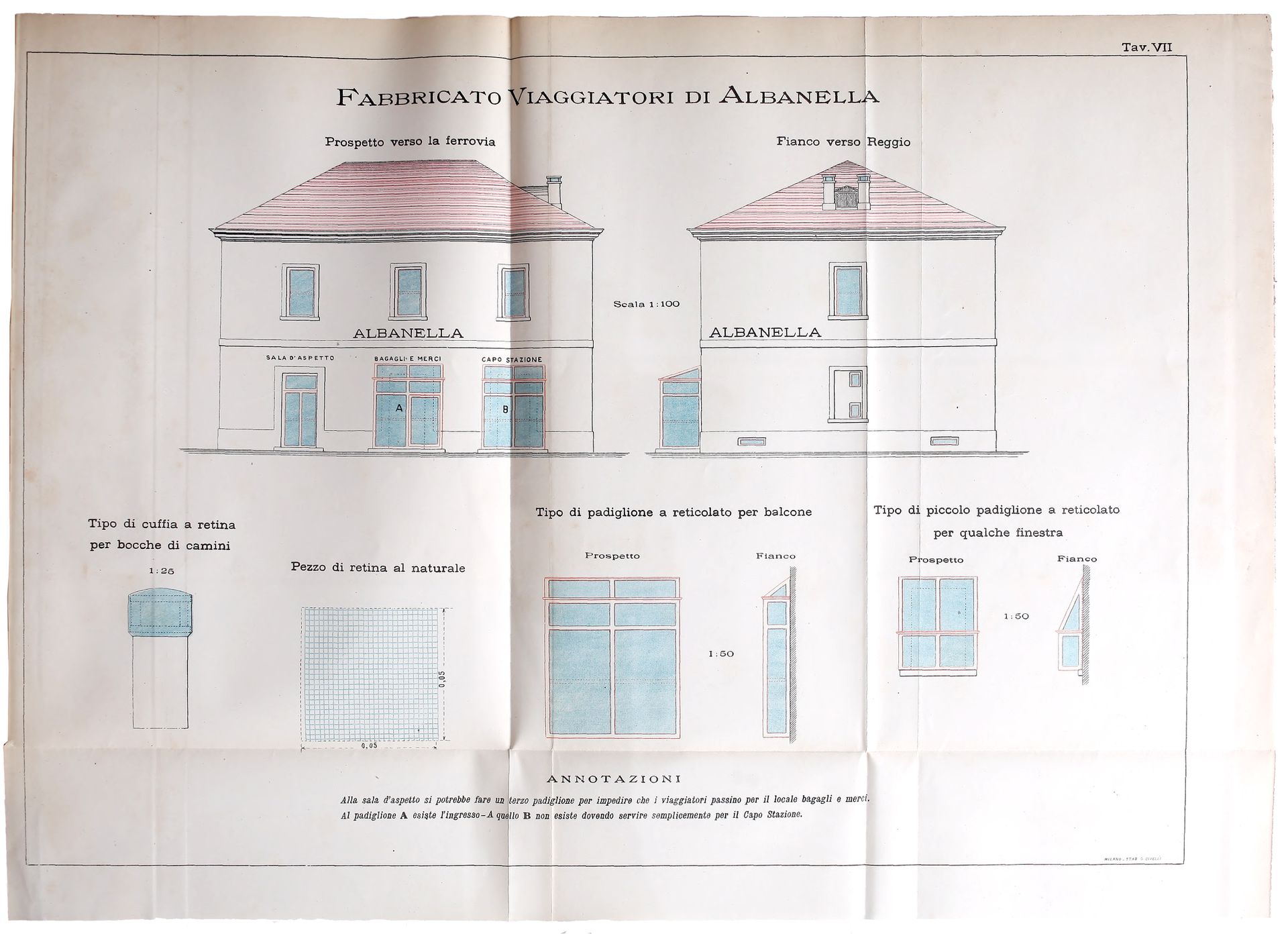
Elevations and details of a train station near Salerno showing anti-mosquito protections, in Giovanni Battista Grassi, Studi di uno zoologo sulla malaria (Rome: 1901), plate 7. Grassi was the first scientist to suggest window screens as a defense against malaria

Collection of blood samples at the anti-malaria school in Nettuno, Rome, 1920. In Giancarlo Majori and Federica Napolitani, eds., Il Laboratorio di Malariologia, (Istituto Superiore di Sanità, 2010), 16
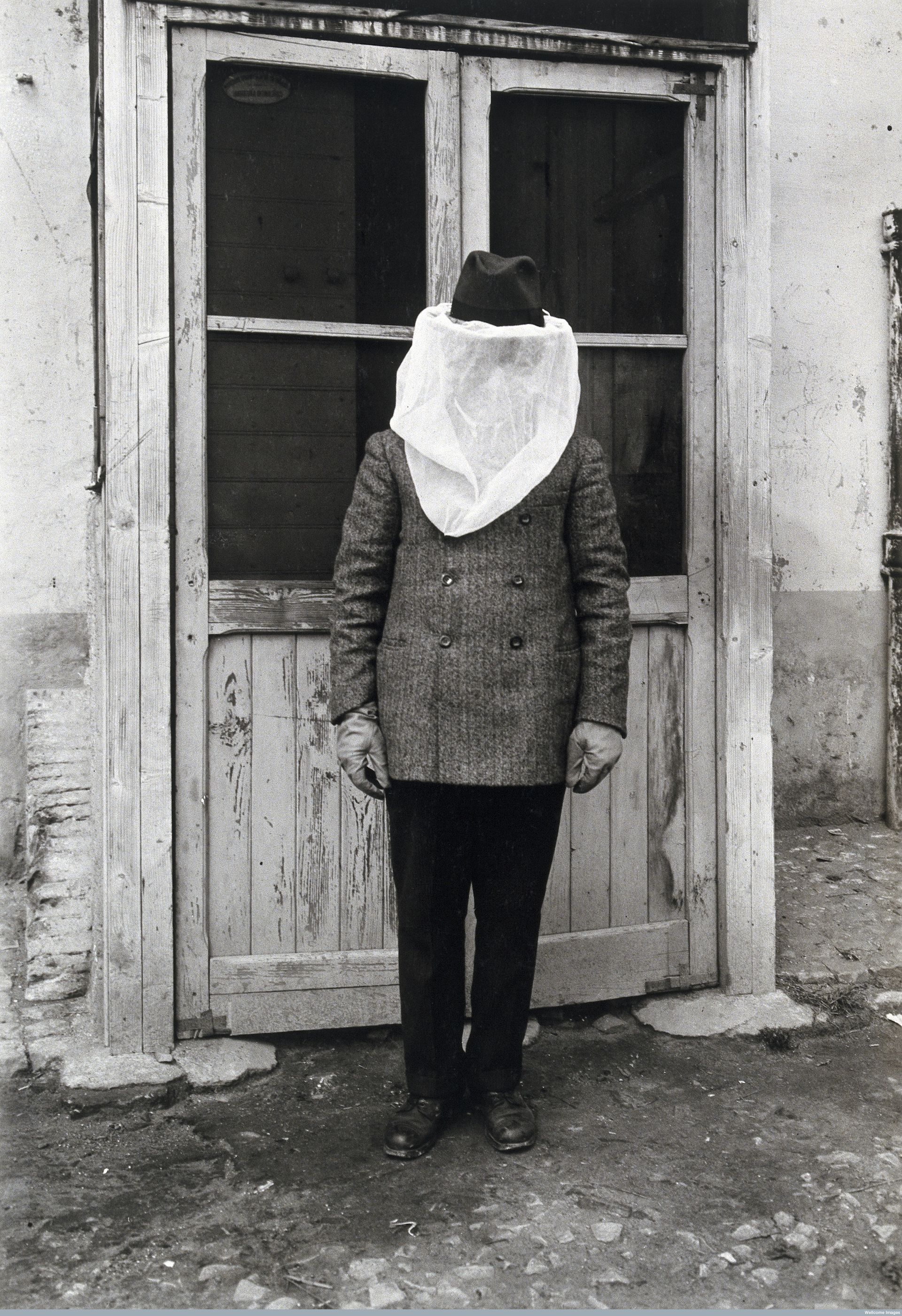
A man wearing mosquito protection at the anti-malaria school in Nettuno, Rome, 1910-1930. Wellcome Library, London
Strategies to control malaria changed again after World War I: Benito Mussolini famously scaled back scientific research and quinine distribution, and instead expanded bonifica. Land reclamation became central to the Fascist narrative, as a way both to make the land productive and, more subtly, to reinforce political consensus among the land-owning bourgeoisie. The reclaimed landscape was a tabula rasa upon which to test a new hygienic architecture and a new form of rural urbanization through planned settlements.
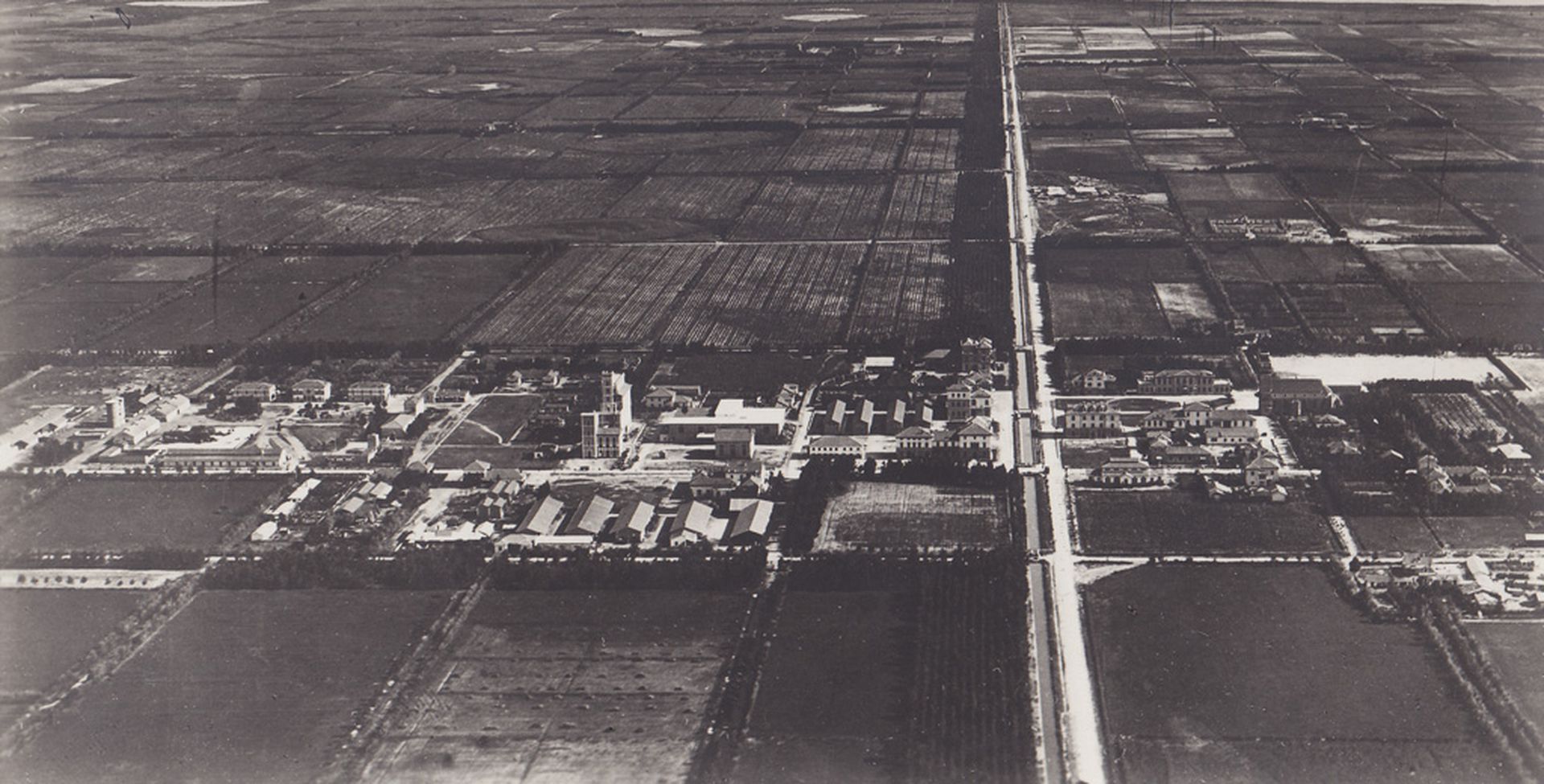
View of Arborea (formerly Mussolinia), a new town founded in 1928 and built on reclaimed land, Sardinia, 1930–1935. Archivio di Stato di Oristano
In its century-long quest to eliminate malaria, Italy remodeled its landscape as a technical and economic project, giving rise to a new anthropogenic nature. Medicalizing the population by means of malarial prophylaxis amounted to the application of a biopolitical technology intended to manage Italy’s new citizens, and their environment, as a singular body.1 Public health served to establish a new territorial order of free circulation that operated beyond the scale of the city. Land reclamation, eucalyptus trees, window screens, quinine distribution, and new towns do not represent a linear evolution, but rather simultaneous strands of an emergent state power and its effect on physical space.
-
Michel Foucault, Society Must Be Defended: Lectures at the Collége de France, 1975–76 (New York: Picador, 2003), 244–247. ↩
This text is part of the long-term research project Terra Infecta, which was started at the Centre for Research Architecture. The project is supported by Het Nieuwe Instituut and the Graham Foundation.